Cochlear Implants
Most children who get a cochlear implant and consistently attend an appropriate speech therapy program will learn to hear, speak and communicate in the same way that their parents communicate.

We expect that these children will go to main-stream school and communicate in the same way as their friends. We find this is the case with many of our patients and pride ourselves on our reputation for success. Unfortunately, not all children will receive this level of benefit from a cochlear implant. We believe it takes a team of hearing specialists (Audiologist, Speech Therapist and Physician) to partner with parents to develop their child’s hearing and communication skills to their full potential.
We hope that the answers to this series of questions will help to guide your family through the cochlear implant process:
Most children who get a cochlear implant and consistently attend an appropriate speech therapy program will learn to hear, speak and communicate in the same way that their parents communicate. We expect that these children will go to main-stream school and communicate in the same way as their friends. Unfortunately, not all children will receive this level of benefit from a cochlear implant. We believe it takes a team of hearing specialists (Audiologist, Speech Therapist and Physician) to partner with parents to develop their child’s hearing and communication skills to their full potential.
What do I do when my child will not wear their cochlear implant?
Children with cochlear implants are no different than children without cochlear implants. All children and teenagers go through periods and phases of development during which they may test their boundaries and limits with their parents. We encourage you to follow the 3 P’s:
- Persistence
- Patience
- Positive Attitude
The Alexander Graham Bell Association for the Deaf and Hard of Hearing has great advise for “Empowering Your Child” with parental advise for practicing the 3 P’s.
What can we do to improve our child’s success with a cochlear implant?
There are many factors that will influence your child’s success with a cochlear implant. Some factors you can control, and some you cannot control. The 3 factors that have the greatest impact on your child’s success that you can control:
- Age at the time your child receives the implant
- Educational and rehabilitation environment that your child is engaged
- Parental involvement
What does cochlear implant surgery involve?
Cochlear implant surgery is completed either as a day surgery (arrive and go home the same day) or as an overnight stay. After completing the registration process at the facility, your child is given a mild sedative in order to aide in any separation anxiety the child may experience. Your child will be in the operating room for approximately 2-1/2 hours. Immediately after surgery, your child will have a large Velcro bandage around the head that will be left on over night (to be removed first thing the morning after surgery). The incision is positioned along the hairline and will measure 3-4cm (about 1.5 inches) in length. A small amount of hair (1-2cm strip or about .5 inches) next to the incision is shaved on the day of the surgery. Once the hair has grown back it is difficult to see or find the scar that is left from the incision.
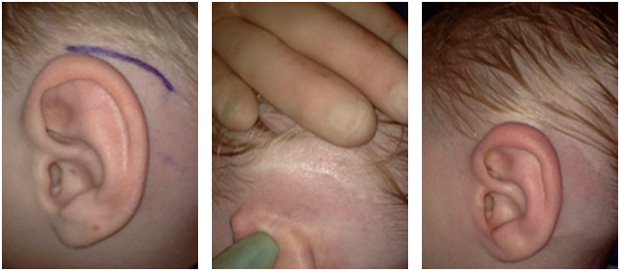
All of the stitches are under the skin (none need to be removed) and the incision line is covered with a substance related to super glue. This area will need to be kept dry for 3 days after surgery. Your child can typically return to normal activities 1 week after surgery.
Is my child a candidate for a cochlear implant?
The criteria for who is an acceptable cochlear implant candidate have evolved over time. We utilize a team approach including and Auditory Verbal Therapist, Audiologist and Physician to help parents establish realistic expectations for their child based on their child’s individual set of circumstances.
Basic Candidacy Criteria for Pediatric Cochlear Implants
- Profound sensorineural hearing loss in both ears
- Child receives little to no benefit from hearing aids
- There are no medical reasons the child cannot undergo surgery
- Child has access to appropriate education and rehabilitation followup after surgery
- Both parent and child are highly motivated to participate in required rehabilitation programs
- Realistic expectations on the part of the parent(s) and, when appropriate, the child.
The criterion for cochlear implant candidacy continues to evolve and expand to include the patients with more residual hearing, one-sided profound hearing loss and other significant medical problems. Ultimately, the goal of the team/program approach to caring for children with hearing loss is to identify children that will not receive or are not receiving sufficient benefit from hearing aids that would be better served by the information provided by a cochlear implant.
What are the communication options for helping my child with severe to profound hearing loss?
Children commonly communicate in many different ways, including facial expressions, gestures, body language and speech. Children with severe to profound degrees of hearing loss were limited to facial expressions, gestures and body language. Cochlear implants have increased the communication options available to children with sever to profound sensorineural hearing loss.
In general, the options for communications include:
- Auditory-Verbal Communication – uses only haring in developing speech and language. The auditory-verbal approach emphasizes parents as the child’s primary teacher, and the focus of the therapy is to provide the parents the tools to teach the child.
- Oral-Aural Communication – emphasizes the use of residual hearing and lip-reading to teach spoken language.
- Cured Speech – combines lip-reading with a system of hand shapes placed near the mouth.
- Sign Language – a visual and manual language using hand shapes and the rest of the body, include the face, to convey words and concepts.
- Total Communications – an approach to rehabilitation that combines the oral-aural and sign language strategies listed above.
While these methods are separate ways of communicating with your child, some parents choose to use them in combination. The mode of communication you use with your child may change over time depending on how well your child uses the hearing aids or cochlear implants and what type of educational programs are available.
Speech therapy following implantation is a critical component to your child’s success using a cochlear implant. The most important predictor of performance after a cochlear implant has been shown to be communication mode*.
In Geers’ study, children in programs that emphasized oral communication were better able to hear, speak and read. In their study sign language did not promote hearing and speech skill development.
*Geers A, Brenner C, Nicholas J, et al. Rehabilitation factors contributing to implant benefit in children. Ann OtolRhinolLarygol (Suppl) 189: 127-130, 2002.
Why does my child have nerve hearing loss?
Congenital hearing loss is our nation’s number one birth defect, with 4 out of every 1000 babies born with moderate to profound permanent nerve hearing loss and 1 out of every 1000 babies born profoundly deaf. Over 90% of children with permanent nerve hearing loss are born to normal hearing parents.
Despite how common this condition is, we still have difficulty in helping parents understand why their child has hearing loss. In fact, as often as 40% of the time, we are unable to establish the reason for a child’s hearing loss.
Reasons for sensorineural hearing loss that can be identified
- Medical History – as part of your child’s initial evaluation we will take a thorough medical history. There are many risk factors that may be identified as par of your child’s medical history that may explain why your child has hearing loss. These risk factors include, but are not limited to, prematurity, NICU stay, oxygen supplementation, intravenous antibiotic Gentamicin, blood transfusion, jaundice (high bilirubin), Chiari malformation.
- Imaging Studies – as part of your child’s evaluation an MRI will be ordered to look at the inner ear structures (cochlea and vestibular system), the nerves that connect the inner ear structures to the brain and the entire brain and brain stem. In some patients structural abnormalities in the inner ear explain why the child has hearing loss. These children are also at an increased risk of progressive hearing loss.
- Genetic Testing – In certain racial and ethnic groups a single genetic condition (Connexi 26) may account for a many as 880% of the cases of sensorineural hearing loss. This and other genetic conditions may be tested as part of your child’s evaluation. Testing typically involves rubbing a swab on the inside of the check. The most common genetic conditions that lead to sensorineural hearing loss are inherited in what is known as a recessive nature. This means that one abnormal gene is inherited from both parents. This also means that you would expect that both parents are not affected by the condition and may have normal hearing
- Depending upon your child’s history and presentation, other studies that may be ordered include: an EKG of the heart, kidney ultrasound, routine blood test and thyroid function test.
What type of hearing loss does my child have?
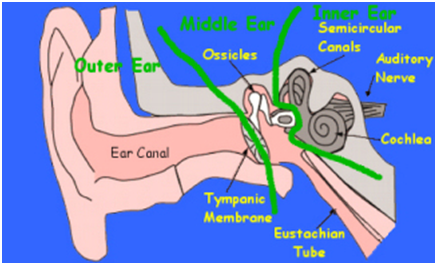
Our ear is divided into 3 parts
- Outer Ear – includes the ear canal and the ear we can see on the outside.
- Middle Ear – the eardrum is the dividing point between the outer and middle ear. The middle ear contains the ossicles.
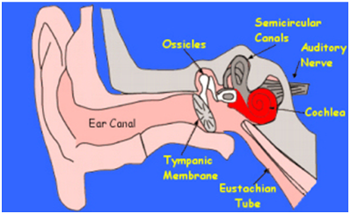
- Inner Ear – includes the cochlea (hearing) and vestibular system (balance).
In general, there are two types of hearing loss:
Conductive Hearing Loss is any process that prevents sound from moving appropriately through the outer or middle ear.
- For example, when a child has an ear infection, fluid accumulates in the middle ear. This limits the movement of sound through the middle ear and creates a conductive hearing loss. This type of hearing loss goes away when the middle ear fluid resolves.
- Another example is a child born without and ear canal (aural atresia). In this example sound cannot move through the ear canal, so even though the inner ear functions normally sound cannot move through the absence ear canal and the child has a conductive hearing loss.
Sensorineural Hearing Loss is an y process that affects the nerve portion of hearing. This includes the inner ear (cochlea), the microscopic hair cells within the cochlea that turn the nerve on and off, the nerve that connects the inner ear to the brain and any part of the hearing pathways within the brain.
- For example, in children with genetic types of sensorineural hearing loss, often the microscopic hair cells within the cochlea that turn the nerve on and off no longer function.
- Another example is a child born without a nerve connecting the inner ear to the brain.
Fortunately, in most children with sensorineural hearing loss, the nerve still functions. It is typically damage to the microscopic hair cells within the inner ear (cochlea) that leads to the hearing loss.
How do we hear?
Normal Hearing: sound comes in through the ear canal
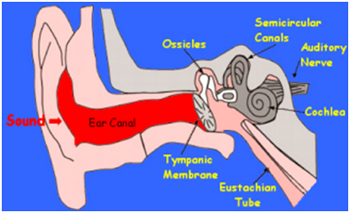
strikes the ear drum (tympanic membrane)
goes across 3 small bones (the ossicles)
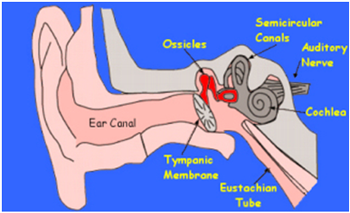
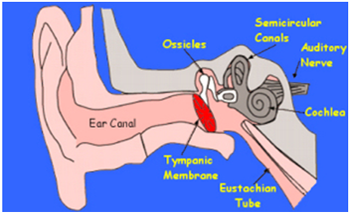
to reach the start of the nerve inside of the cochlea
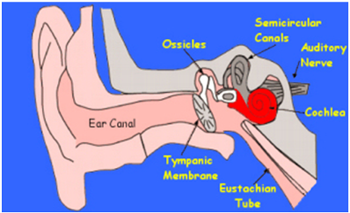
Inside the cochlea there are two types of microscopic hairs: Inner and outer Hair Cells
Once the sound wave reaches the cochlea the outer hair cells are activated.
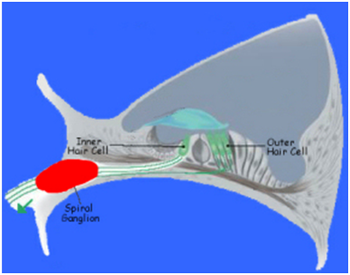
The outer hair cells act like a switch and turn the nerve (spiral ganglion) on and off. The sound wave now becomes a nerve impulse.
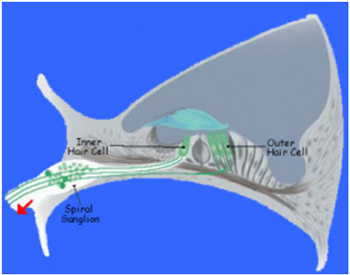
From the spiral ganglion cell, the nerve impulse is transported along the auditory nerve to the brain.
A cochlear implant stimulates the spiral ganglion cell directly to create the nerve impulse. The cochlear implant is bypassing the hair cells.
What is a cochlear implant and how does a cochlear implant work?
In children with severe to profound sensorineural hearing loss, hearing aids provide little or no benefit. A cochlear implant system bypasses the non-functioning part of the cochlea and delivers sound signals directly to the hearing nerve. Cochlear implants are hearing devices that take over the function of the damaged hair cells in the inner hear.
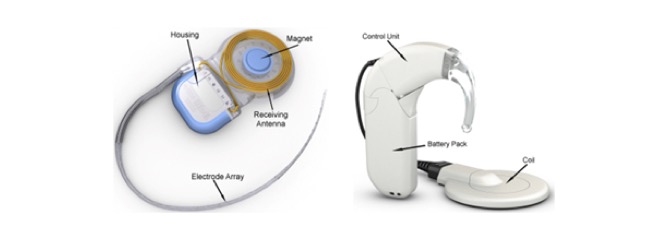
A cochlear implant system is composed of 2 general parts:
- Internal – the internal portion is the “implant” that is surgically placed under the skin. The implant consists of a housing, which contains the electronics, and the electrode array as well as the receiving antenna and a magnet that holds the coil in place behind the ear.
- External – the external portion is the “Processor” that is worn behind the ear. The audio processor consists of a control unit that houses the microphone, a battery pack, and a coil that transmits information through the skin to the implant.
Cochlear implants can be used effective by children who are deaf at birth and by children who become deaf later in life.
How Does a Cochlear Implant Work?
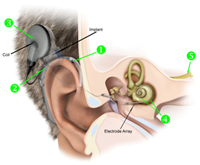
- A cochlear implant system has a microphone that collects everyday sounds and converts the sound into an electrical signal.
- The is signal is sent to the speech processor where it is “coded” (turned into a special patter of electrical pulses).
- The coded electrical impulses are sent to the coil and are then transmitted across the intact skin to the implant.
- The implant sends a pattern of electrical pulses to the electrodes in the cochlea.
- The auditory hearing nerves (spiral ganglion cells) pickup the electrical pulses and send them to the auditory center in the brain. The brain recognizes these electrical signals as sound.